Selective Functional Movement Assessment (SFMA Top Tier) Reliability, Validity, Procedure and Normative Data
By Sophia Miller, SPT & Phil Plisky, PT, DSc, ATC, CSCS
Top Tier SFMA Protocol
The Top Tier Selective Functional Movement Assessment (SFMA) consists of a series of 10 screening patterns to assist practitioners in identifying dysfunctional and painful movements.
Without warming up, the person should remove their shoes, stand with their feet together, and perform the specified movement. These movements consist of:
- Cervical Flexion
- Cervical Extension
- Cervical Rotation
- Upper Extremity Pattern 1 (Extension and Internal Rotation)
- Upper Extremity Pattern 2 (Flexion and External Rotation)
- Multi-Segmental Flexion
- Multi-Segmental Extension
- Multi-Segmental Rotation
- Single Leg Stance
- Arms Down Deep Squat
For detailed procedures and scoring, see Functional Movement Systems Selective Functional Movement Assessment Academy Course
Scoring the Top Tier SFMA
The rater grades the movement patterns according to reproduction of pain and level of functionality as “Functional, Nonpainful”, “Functional, Painful”, “Dysfunctional, Nonpainful”, or “Dysfunctional, Painful”. Any patterns not meeting the “Functional, Nonpainful” criteria can then be further broken down to identify the root cause(s) of the dysfunctional movement.
What is the Reliability of the SFMA?
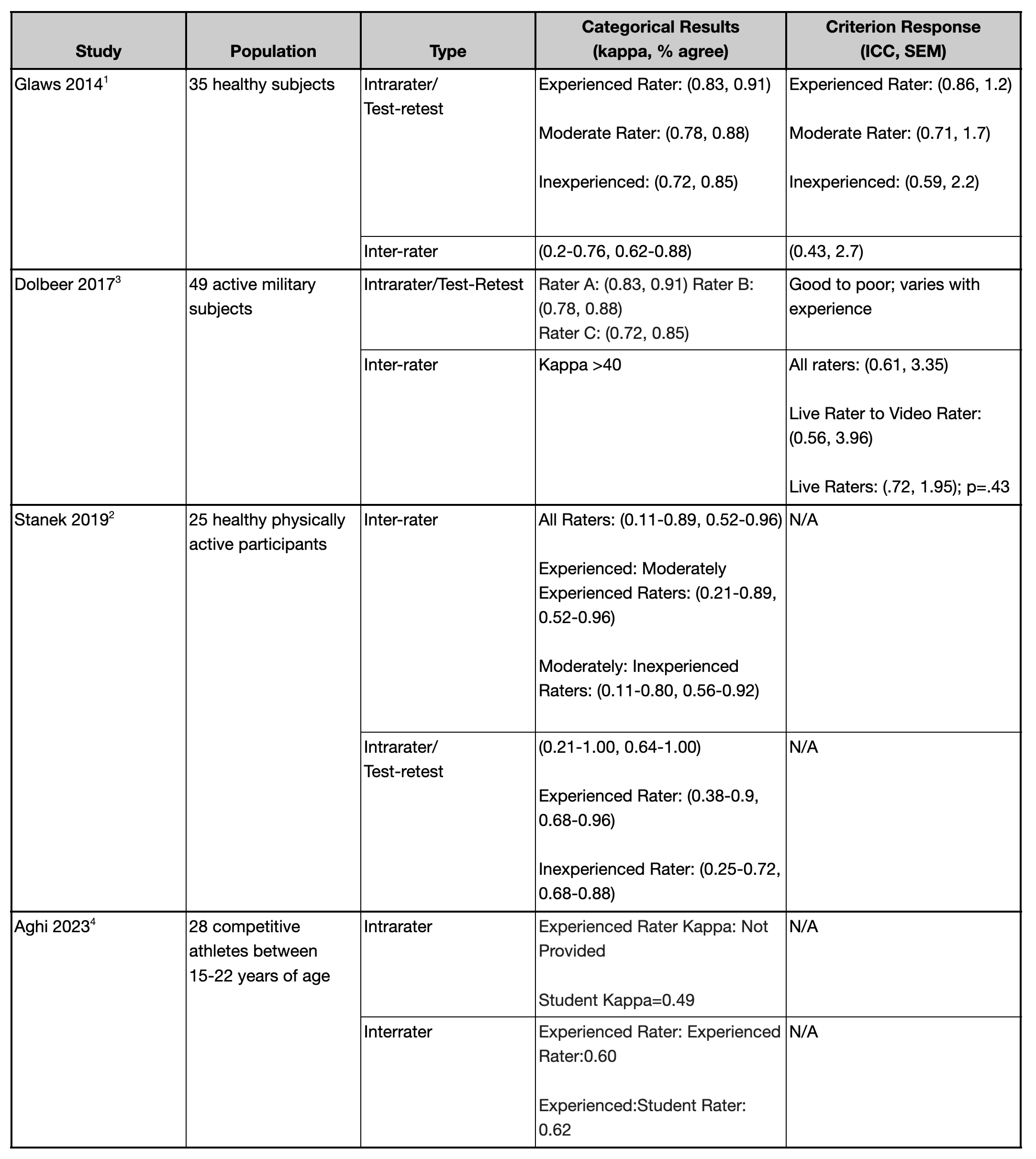
When comparing the intra-rater reliability kappa values of the categorical Top Tier SFMA, Glaws et al1 found that more experienced raters have almost perfect agreement while less experienced graders have fair to substantial agreement. Dolbeer et al3 revealed that the categorical scoring tool proved to have better interrater and intrarater reliabilities, and Stanek and Dolbeer2 agreed that more experienced raters had higher intrarater reliability with the categorical grading of the Top Tier SFMA. Aghi et al4 found that rater experience does not make a large difference in inter-rater reliability, but rather that some movements were more reliably scored. Most studies tend to agree that more experienced graders have more reliable results with the Top Tier SFMA.1,2
When comparing the two grading forms, the Categorical Results yielded higher inter-rater reliability than the Criterion Response, which is expected when analyzing human movement.1,3
Top Tier SFMA Reliability
What is the Validity of the Top SFMA?
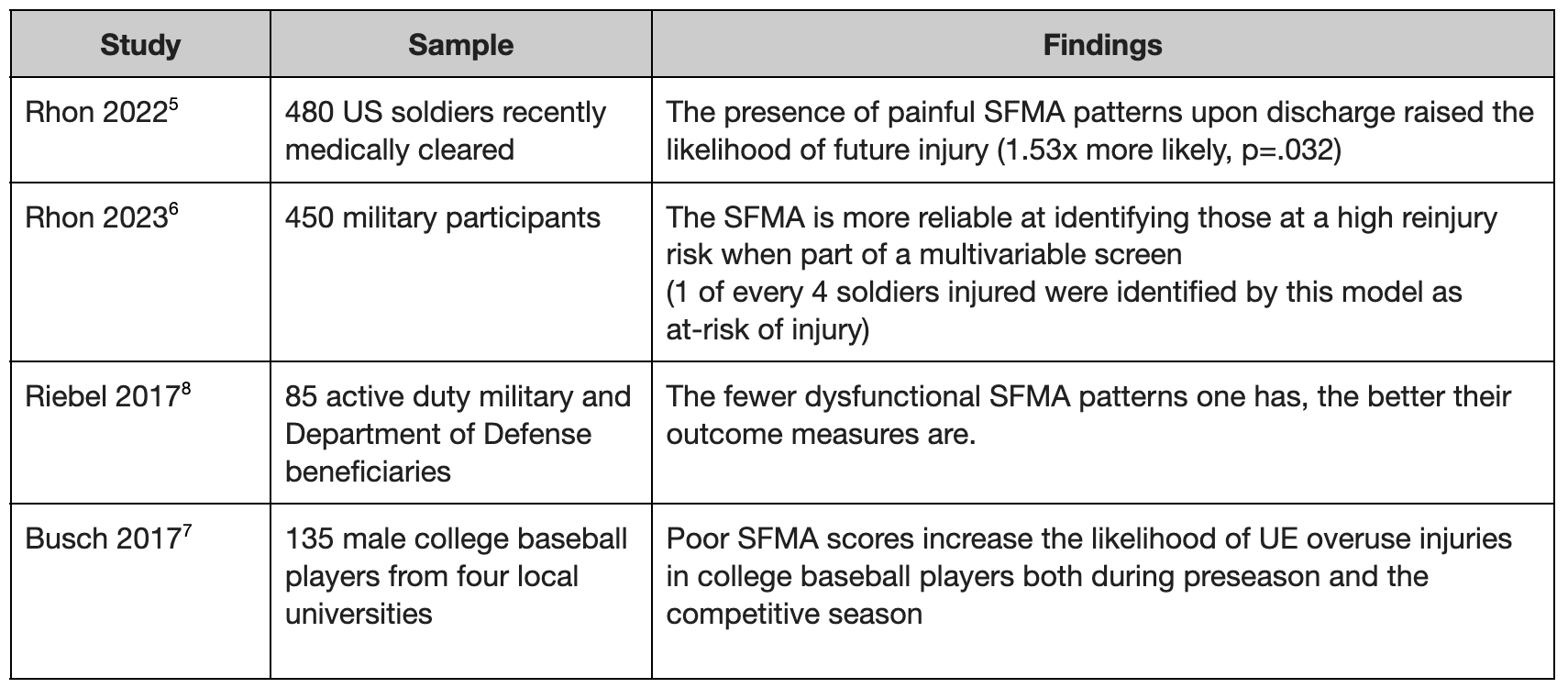
The SFMA effectively identifies poor patterns of motion that leave patients exposed to reinjury. If left unaddressed, these inappropriate patterns make a person 1.5x more likely to encounter a future injury, yet movement pattern testing is often skipped over in the discharge process.5
Rhon et al. found that ¼ of soldiers who had subsequent injuries had been correctly identified by the SFMA as at-risk of reinjury, demonstrating that the SFMA to be a limited, but nonetheless successful tool in identifying those most at risk for reinjury and therefore unfit to be medically cleared.6
Additionally, Busch et al. found that players with poor SFMA performances were more likely to experience overuse symptoms or injuries.7 This research suggests that the UE patterns of the SFMA correlate to the likelihood of overuse injuries in college baseball players as they found that players with worse SFMA performances were more likely to report preseason (OR: 6.10) or in season (OR: 17.07) overuse symptoms in their shoulders or elbows.7
A 2017 study discovered that a decrease in the number of SFMA painful patterns correlated with an improvement in the commonly used self-reported outcome measures for pain, function, and disability.8 This study supports the use of the SFMA a testing tool can identify people not truly ready to return to activity and prevent possible reinjury from rejoining their sport too soon.8
Validity of Top Tier SFMA
About the Co-Author
Sophia Miller, SPT
Sophie is an Exercise Physiologist and current Physical Therapy student at the University of Evansville with a passion for athletics and sports rehabilitation. She is the Head of Performance and Rehabilitation for the UPSL’s Midwest Hooligans and is entering her 4th season with the team.
References
- Glaws KR, Juneau CM, Becker LC, Di Stasi SL, Hewett TE. Intra- and inter-rater reliability of the selective functional movement assessment (sfma). Int J Sports Phys Ther. 2014;9(2):195-207.
- Stanek JM, Smith J, Petrie J. INTRA- AND INTER-RATER RELIABILITY OF THE SELECTIVE FUNCTIONAL MOVEMENT ASSESSMENT (SFMA) IN HEALTHY PARTICIPANTS. Int J Sports Phys Ther. 2019;14(1):107-116.
- Dolbeer J, Mason J, Morris J, Crowell M, Goss D. INTER-RATER RELIABILITY OF THE SELECTIVE FUNCTIONAL MOVEMENT ASSESSMENT (SFMA) BY SFMA CERTIFIED PHYSICAL THERAPISTS WITH SIMILAR CLINICAL AND RATING EXPERIENCE. Int J Sports Phys Ther. 2017;12(5):752-763.
- Aghi A, Salvagnini D, Berton G, et al. Selective Functional Movement Assessment (SFMA) Reliability and Proposal of Its Use in Sports. International Journal of Environmental Research and Public Health. 2023;20(3):2032.
- Rhon DI, Teyhen DS, Kiesel K, et al. Recovery, Rehabilitation, and Return to Full Duty in a Military Population After a Recent Injury: Differences Between Lower-Extremity and Spine Injuries. Arthrosc Sports Med Rehabil. 2022;4(1):e17-e27.
- Rhon DI, Plisky PJ, Kiesel K, et al. Predicting Subsequent Injury after Being Cleared to Return to Work from Initial Lumbar or Lower Extremity Injury. Med Sci Sports Exerc. 2023;55(12):2115-2122.
- Busch AM, Clifton DR, Onate JA, Ramsey VK, Cromartie F. RELATIONSHIP OF PRESEASON MOVEMENT SCREENS WITH OVERUSE SYMPTOMS IN COLLEGIATE BASEBALL PLAYERS. Int J Sports Phys Ther. 2017;12(6):960-966.
- Riebel M, Crowell M, Dolbeer J, Szymanek E, Goss D. CORRELATION OF SELF-REPORTED OUTCOME MEASURES AND THE SELECTIVE FUNCTIONAL MOVEMENT ASSESSMENT (SFMA): AN EXPLORATION OF VALIDITY. Int J Sports Phys Ther. 2017;12(6):931-947.








